
Abstract
Background: Several methods have been used to prevent
post spinal hypotension including preloading, co-loading,
use of vasopressors, placement of pelvic wedge, lumbar
wedge and tilting of operating table in parturients undergoing
cesarean section. We conducted a randomized controlled
study to determine the hemodynamic effects of a standard
pelvic wedge placed below the right hip immediately after
the spinal block till the delivery of baby.
Methods: One hundred consenting women undergoing
elective cesarean section under spinal anesthesia were
randomly allocated to wedge group (N=50) and control
group (N=50). A standard wedge was placed under the
right pelvis soon after spinal anesthesia till the delivery of
baby in wedge group whereas the control group remained
supine. Hemodynamic parameters including blood pressure,
heart rate, vasopressor consumption, other side effects like
nausea, vomiting and neonatal outcome were also recorded.
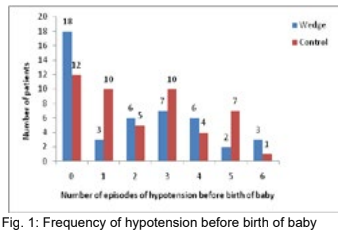
Results: The incidence of hypotension and bradycardia
was similar between groups (Wedge group 60% vs Control
group 75.51%, p=0.125) before the birth of baby. The use of
vasopressors (p=0.212), incidence of nausea (p=0.346) and
Apgar score at 1 and 5 minutes (p=0.629, p=0.442) were
also not statistically significant. None of the patients had
vomiting.
Conclusion: In our study, the use of right pelvic wedge
immediately after spinal anesthesia was not effective in
preventing post spinal hypotension in elective cesarean
section.
References
section: a survey of practice. Anaesthesia. 2001;56(8):794–8.
2. Mercier FJ, Augè M, Hoffmann C, Fischer C, Le Gouez A. Maternal hypotension during spinal anesthesia for caesarean delivery.
Minerva Anestesiol. 2013;79(1):62–73.
3. Apfelbaum JL, Hawkins JL, Agarkar M, Bucklin BA, Connis RT, Gambling DR, et al. Practice Guidelines for Obstetric Anesthesia:
An Updated Report by the American Society of Anesthesiologists Task Force on Obstetric Anesthesia and the Society for Obstetric
Anesthesia and Perinatology. Vol. 124, Anesthesiology. 2016. 270-300 p.
4. Gurumeta AA, Vecino JMC. Colloids versus crystalloids in the prevention of cesarean section . A systematic review and meta-
analysis. Minerva Anestesiol. 2015;81(9):1019–30.
5. Bamber JH, Dresner M. Aortocaval Compression in Pregnancy: The Effect of Changing the Degree and Direction of Lateral Tilt on
Maternal Cardiac Output. Anesth Analg. 2003;97:256–8.
6. Morgan PJ, Tarshis J, Halpern SH. The Effects of an Increase of Central Blood Volume Before Spinal Anesthesia for Cesarean
Delivery: A Qualitative Systematic Review. Anesth Analg. 2001;92(January):997–1005.
7. Law ACS, Lam KK, Irwin MG. The Effect of Right Versus Left Lateral Decubitus Positions on Induction of Spinal Anesthesia for
Cesarean Delivery. Anesth Analg. 2003;97:1795–9.
8. Kundra P, Arunsekar G, Vasudevan A, Vinayagam S, Habeebullah S. Effect of postural changes on inferior venacava dimensions
and its influence on haemodynamics during caesarean section under spinal anaesthesia Effect of postural changes on inferior vena
cava dimensions and its infl uence on haemodynamics during caesar. J Obstet Gynaecol (Lahore). 2015;35(7):667–71.
9. Hasanin A, Aiyad A, Elsakka A, Kamel A, Fouad R, Osman M, et al. Leg elevation decreases the incidence of post-spinal hypotension
in cesarean section : a randomized controlled trial. BMC Anesthesiol. 2017;17(60):1–6.
10. Mendonca C, Griffiths J, Ateleanu B, Collis RE. Hypotension following combined spinal-epidural anaesthesia for Caesarean section:
Left lateral position vs. tilted supine position. Anaesthesia. 2003;58(5):428–31.
11. Kinsella SM, Whitwam JG, Spencer JA. Reducing aortocaval compression: how much tilt is enough? BMJ [Internet].
1992;305(6853):539–40. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1883291/pdf/bmj00090-0009.pdf
12. Cluver C, Novikova N, Gj H, Cluver C, Novikova N, Hofmeyr GJ, et al. Maternal position during caesarean section for preventing
maternal and neonatal complications ( Review ) Maternal position during caesarean section for preventing maternal and neonatal
complications. Cochrane database Syst Rev. 2013;(3):3–5.
13. Todris L, Etchin A, Kuint J. Maternal hypotension during elective cesarean section and short-term neonatal outcome. Am J Obstet
Gynecol [Internet]. 2010;202(1):56.e1-56.e5.Available from: http://dx.doi.org/10.1016/j.ajog.2009.07.012
14. Stoneham M, Eldridge J, Popat M, Russell R. Oxford positioning technique improves haemodynamic stability and predictability of
block height of spinal anaesthesia for elective caesarean section. Int J Obstet Anesth. 1999;8:242–8.
15. Lewis NL, Ritchie EL, Downer JP, Nel MR. Left lateral vs. supine, wedged position for development of block after combined spinal-
epidural anaesthesia for Caesarean section. Anaesthesia. 2004;59(9):894–8.
16. Hartley H, Seed PT, Ashworth H, Kubli M, O’Sullivan G, Reynolds F. Effect of lateral versus supine wedged position on development
of spinal blockade and hypotension. Int J Obstet Anesth. 2001;10(3):182–8.
17. Rees SGO, Thurlow JA, Gardner IC, Scrutton MJL, Kinsella SM. Maternal cardiovascular consequences of positioning after spinal
anaesthesia for Caesarean section: Left 15° table tilt vs. left lateral. Anaesthesia. 2002;57(1):15–20.
18. Calvache JA, Muñoz MF, Baron FJ. Hemodynamic effects of a right lumbar-pelvic wedge during spinal anesthesia for cesarean
section. Int J Obstet Anesth. 2011;20(4):307–11.
19. Zhou ZQ, Shao Q, Zeng Q, Song J, Yang JJ. Lumbar wedge versus pelvic wedge in preventing hypotension following combined
spinal epidural anaesthesia for caesarean delivery. Anaesth Intensive Care. 2008;36(6):835–9.