
Abstract
Background:
Chronic otitis media (COM) squamous type is commonly as-sociated with cholesteatoma. In COM squamous type with active disease, there is retraction of pars flaccida or pars tensa with retention of squamous epithelial debris and is associated with inflammation and production of pus. It is potentially dangerous because it can cause resorption of bone, leading to ossicular erosion and destruction of bony plates of middle ear. The objective of this study is to determine the effect of chronic otitis media squamous typeon the ossicular chain as well as to observe the types of pathology in this disease.
Methods and materials:
Fifty cases of chronic otitis media squamous type who underwent surgical management were included. The status of ossicular chain was evaluated intraoperatively. The type of pathology involving middle ear was also studied. Cases admitted for revision surgery were excluded from the study.
Results:
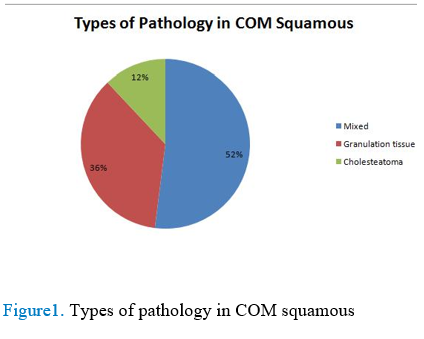
Of the total fifty cases, ossicular changes were observed in forty eight cases and in two cases all ossicles were
intact. Long process of incus is the most frequently involved ossicle. The most common pathology was found to be mixed type (52%).
Conclusion:
The conclusion of this study is that ossicular chain is commonly involved in chronic otitis media squamous type and mixed pathology consisting of cholesteatoma and granulation tissue is the most frequent pathology.
References
Hodder Arnold; 2008. p. 3410.
2. Dhingra PL. Cholesteatoma and chronic suppurative otitis media. In: Dhingra PL. Diseases of ear, nose and throat. 4th ed. New Delhi: Elsevier; 2007. p. 66-72.
3. Slaterry WH. Pathology and clinical course of inflammatory diseases of middle ear. In: Glasscock ME, Gulya AJ. Glass-cock-Shambaugh Surgery of the ear. 5th ed. New Delhi: Elsevier; 2003:429.
4. Browning GG, Merchant SN, Kelly G, Swan IRC, Canter R, Mck-errow WS. Chronic otitis media. In: Gleeson M. Scott-Brown’s otorhinolaryngology, head and neck surgery. 7th ed. London:
Hodder Arnold; 2008.p. 3395-434.
5. Mills RP. Management of chronic suppurative otitis media. In: Kerr AG, Booth JB. Scott-Brown’s Otolaryngology. 6th ed. Ox-ford: Butterworth Heinemann; 1997. p. 3/10/1.
6. Evandro J, Alvares N, Negro J. Choleateatoma surgery in children and adolescents: analysis in 200 patients. International archives of otorhinolaryngology 2006; 10(1).
7. Nikolopoulos TP, Gerbesiotis P. Surgical management of cho-lesteatoma:the two main options and the third way-atticotomy/ limited masoidectomy. Int J PediatrOtorhinolaryngol 2009; 73(9):1222-7.
8. Kveton JF. Open cavity mastoid operations. In: Glasscock
ME,Gulya AJ. Surgery of the ear. 5th ed. New Delhi: Elsevier; 2003.p. 499-15.
9. Shrestha S ,Kafle P. Intraoperative findings during canal wall down mastoidectomy in children. Journal of Nepal Paediatric So-ciety 2011; 31(3):184-7.
10. Chalise SR, Bhandary S. Chronic suppurative otitis media ‘unsafe type’: an experience at a tertiary care hospital. Nepalese J ENT
Head Neck Surg 2013; 4(1): 23-5.
11. Kumar RV, Koribipati NK, Krishna RN, Indira S, Ramakrishnan P. Infection and ossicular necrosis in atticoantral disease. Otolar-yngology online journal. 2015; 5(1).
12. Semaan MT, Megerian CA. The pathophysiology of cholesteato-ma. OtolaryngolClin N Am 2006;39:1143-59.
13. Chole RA, McGinn MD, Tinling SP. Pressure-induced bone re-sorption in the middle ear Ann OtolRhinolLaryngol 1985;94(2 Pt 1):165–70.
14. Burger EH, Klein-Nulen J. Responses of bone cells to biome-chanical forces in vitro. Adv Dent Res 1999;13:93–8.
15. Jung JY, Pashia ME, Nishimoto SY, et al. A possible role for nitric oxide in osteoclastogenesis associated with cholesteatoma.
OtolNeurotol 2004;25(5):661–8.
16. Yan SD, Huang CC. The role of tumor necrosis factor-alpha in bone resorption of cholesteatoma. Am J Otolaryngol 1991;
12(2):83–9.
17. Klein-Nulend J, van der Plas A, Semeins CM, et al. Sensitivi-ty of osteocytes to biomechanical stress in vitro. FASEB J
1995;9(5):441–5.
18. Albera R, Canale A, Piumetto E, Lacilla M, Dagna F. Ossicular chain lesions in cholesteatoma. Acta Otorhinolaryngologica Itali-ca 2012;32:309-13.
19. Salman AA, Azhar K, Muhammad EK , Muhammad M. Analyt-ical study of ossicular chain in middle ear cholesteatoma. King Edwards Medical University Annals 2009; 15(3):134-7.
20. Mohammadi G, Naderpour M, Mousaviagdas M. Ossicular ero-sion in patients requiring surgery for cholesteatoma. Iranian Jour-nal of Otorhinolaryngology 2012; 24(3):125-8.