
Abstract
Introduction: Haematuria is one of the most
common presentations of renal disease Urinary
sediment examination by urine phase contrast
microscopy (PCM) is a useful diagnostic marker
for glomerular bleeding if correctly interpreted
and used. Although PCM is simple and cost
effective the percentage of dysmorphic red cells
regarded as diagnostic of glomerular haematuria
is controversial and varied from (10-90)% cases in
different series. This study is done with the aim to
evaluate urine phase contrast microscopy as a tool
in differentiating glomerular haematuria in patients
with glomerulonephritis confirmed by renal biopsy
and non-glomerular haematuria in patients with
renal stone disease.
Materials and Methods: In this study, 175 patients
with haematuria were taken and were divided
into two groups; Group I with diagnosed
cases of glomerulonephritis with haematuria
confirmed with renal biopsy and Group II with
patients of renal stone disease with haematuria.
After diagnosing haematuria, all patients were
undergone for urine phase contrast microscopy.
Renal biopsy was done in patients suspected for
glomerulonephritis.
Results: This study showed that the mean
percentage of dysmorphic RBCs in group I by
urine PCM was (35.8%) which was significantly
higher than in group II (6.8%). A comparison
was done between the different cut off values for
percentages of dysmorphic RBCs to differentiate
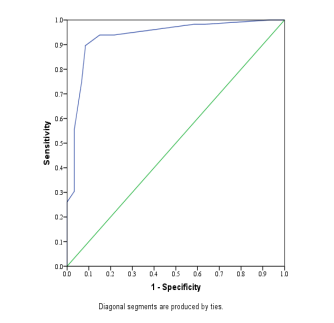
glomerular from non-glomerular haematuria. For
a cut off value of 20%, the present study showed
the most agreeable sensitivity 80.7% and specificity
90.6%.Receiver-operator characteristic curve for
percentage of dysmorphic RBCs, area under the
curve was 0.934, which gave an optimal sensitivity
80.7% and specificity 90.6% for a decision level
cut off of 20% dysmorphic RBCs. It was found
that patients of group I had higher serum creatinine
level (mean 1.6 mg/dl) in comparison to group
II (mean 1.1mg/dl). Similarly patient of group
I had higher level of proteinuria in comparison
to group II. It was also ovbserved that patients
with proliferative glomerulonephritis had higher
percentage of dysmorphic RBCs in comparison
to non-proliferative type of glomerulonephritis.
Conclusion: Urine phase contrast microscopy
is a simple, cost effective, non invasive and
reliable investigation. Patients with proliferative
glomrulonephritis may have a higher percentage of
dysmorphic RBCs in comparison to those with non
proliferative glomerulonephrits.
References
method for identifying glomerular bleeding. Kidney
Int; 1982 21: 105±10.
2. Dinda AK, Saxena S, Guleria S, Tiwari SC, Dash
SC, Srivastava RN, et al. Diagnosis of glomerular
haematuria:role of dysmorphic redcell, G1cells and
brightfield microscopy. Scand J Clin Lab Invest;
1997.57: 203-8.
3. .Turner P. Renal biopsy in a general hospital. J
ClinPathol; 1963 16: 448-51
4. Abolfathi A, Hosaininasab A, Argani H.
Differentiation of glomerular from non-glomerular
haematuria by three different methods of
microscopic examinations of erythrocytes in urine.
IJMS; 2007. 32(3): 163-8.
5. Swaminathan S, Nelson Leung, Donna J Lager,
L Joseph Melton 3rd, et al. Changing Incidence of
Glomerular Disease in Olmsted County, Minnesota:
A 30-year Renal Biopsy Study. Clin J Am Soc
Nephrol. 2006 May; 1(3):483-7.
6. P.V. Bottini; C.R. Garlipp; J.R. Lauand; S.G. Lara
Cioffi; S.H. Afaz; R. Lopes Prates Glomerular and
Non-Glomerular Haematuria: Preservation of Urine
Sediment.Lab Med. 2005;36(10):647-649
7. Mohammad KS, Bdesha AS, Snell ME, Witherow
RON, Coleman DV. Phase contrast microscopic
examination of urinary erythrocytes to localize
source of bleeding: an overlooked technique?
ClinPathol; 1993. 46: 642
8. Pollock C, Pei-Ling L, Gyory AZ, Grigg R,
Gallery ED, Caterson R, et al. Dysmorphism of
urinary red blood cells- value in diagnosis. Kidney
Int; 1989.36: 1045-9.
9. Rizzoni G, Braggion F, Zaechelio G. Evaluation
of glomerular and non-glomerular hematuria by
phasecontrast microscopy. J Pediatr; 1983. 103:
370
10. Roberto SC, Souza RMB, Franco PB, Dantas M,
Gomes UA, Reis MA, “Evaluation of erythrocyte
morphology in the urinary sediment for the
differential diagnosis of haematuria using standard
light microscopy” Nephrology,vol.2, pp. 1996, 181-
185
11. Alam MR, Khanam A, Alam KS, Muqueet MA,
Rahman H, Rashid HU. Prevalance of comorbidity
in haemodialysis patient. Bangladesh Renal J;
2004.23(2): 56-60
12. Brich DF, Fairly KF, Witworth JA, Forbes IK et
al. Urinary morphology in diagnosis of glomerular
haematuria. ClinNephrol; 1983. 20:78-84.
13. Sparwasser C, Cimniak HU, Treiber U, Pust
RA. Significance of the evaluation of asymptomatic
microscopic haematuria in young men. Br J Urol.;
1994. 74:723–729.
14. Sultana T, Rahman MQ, Rahman F, Islam MS,
Ahmed ANN. Value of dysmorphic red cells and G1
cells by phase contrast microscopy in the diagnosis
of glomerular diseases. Mymensingh Med J; 2011.
20(1): 71-7.
15. Thomas J. Pillsworth, Jr.,1 Virginia M. Haver,
Christine K. Abrass,2and Coliene J. Delane
Differentiation of Renal from Non-Renal Hematuria
by Microscopic Examination of Erythrocytes in
Urine Clin. Chem.1987. 33/10, 1791-1795